Journal of Medicine and Life Vol. 9, Issue 2, April-June 2016, pp.177-179
Gheorghe A*, Pop M**, Burcea M**, Serban M***
*“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
**Clinical Emergency Eye Hospital, Bucharest, Romania
***”Victor Anastasiu” National Institute for Aeronautical and Spatial Medicine, Bucharest, Romania
Correspondence to: Zemba M, MD, PhD,
Ophthalmology Department, Central Military Emergency University Hospital, Bucharest,
134 Calea Plevnei Street, Bucharest, Romania,
Phone: +4021 3137189, E-mail: mhlzmb@yahoo.com
Received: December 14th, 2015 – Accepted: March 7th, 2016
Abstract
Abstract
The new defined anatomical and functional complex conjunctiva-limbus-cornea is a new concept, which helps clinicians better understand and treat ocular surface pathologies. The management of the ocular surface disease has changed dramatically over the years, with spectacular improvements of techniques, and of course, results. The amniotic membrane, used as a graft or as a substrate for the cultivation of limbal corneal cells has showed encouraging results.
Aim: To investigate the usefulness of amniotic membrane transplantation in ocular surface pathologies.
Method: The study is retrospective. 28 eyes of 28 patients with ocular surface pathologies (ocular burns, recent and old, symblepharon, pterygium, corneal and conjunctival tumors, persistent epithelial defect) underwent an amniotic membrane transplantation during a 1 year period. The necrotic and the scar tissue were first excised in all the patients and the amniotic membrane was sutured with an epithelial face up. Follow up ranged from 1 to 12 months.
Results: Good results were obtained in all 28 eyes. The anatomy of cornea and conjunctiva was improved, with limited benefits only in old ocular burn, symblepharon and in one case of extended tumors of the cornea and conjunctiva. Out of 28 eyes, 23 (82%) also had a visual acuity improvement.
Conclusion: The amniotic membrane may be considered a good alternative for ocular surface reconstruction especially in acute status.
Keywords: ocular surface, amniotic membrane transplantation, limbal stem cells deficiency
Abbreviations: AMT = amniotic membrane transplantation, BCVA = best corrected visual acuity, BUT = break up time
Method
Our study was conducted on 28 eyes of 28 patients. 9 of them had alkali burns, 5 were recent and 4 were old. 2 patients had symblepharon, 6 pterygium with important corneal invasion. We also enrolled 8 patients with tumors of the cornea and conjunctiva, 2 of them presenting a large invasion of the surrounding tissue, a persistent epithelial defect in 1 young patient without any other systemic pathologies and diabetes mellitus in 2 patients. All the patients complained of photophobia, epiphora, decreased visual acuity, and poor cosmetic status. BCVA ranged from LogMAR 0 to LogMAR 1 in patients with severe corneal tumors, symblepharon and old alkali burns. All the patients were carefully examined at the ocular slit biomicroscope. Schirmer tests, BUT tests and corneal staining with fluorescein examination for corneal epithelial defects were performed. Before the surgery, all the patients filled a questionnaire ranging the score of their photophobia and general ocular discomfort. The amniotic membrane was carefully prepared and after the removal of necrotic or scaring tissue of the patient, it was sutured, on the eye, with epithelial face up. After surgery, the patients were examined at 1, 7, 14 days and then monthly. They were asked to fill in the questionnaire again 1 month after the surgery.
These individual data were analyzed and results were reported in percentage or absolute numerical value.
Results
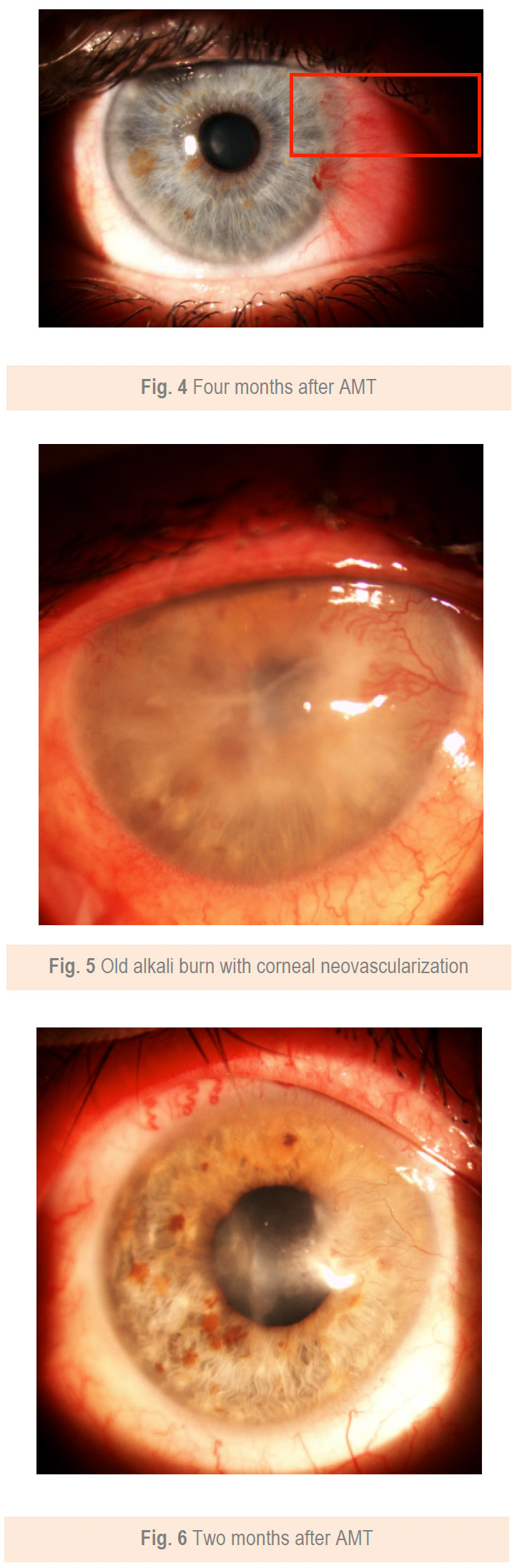
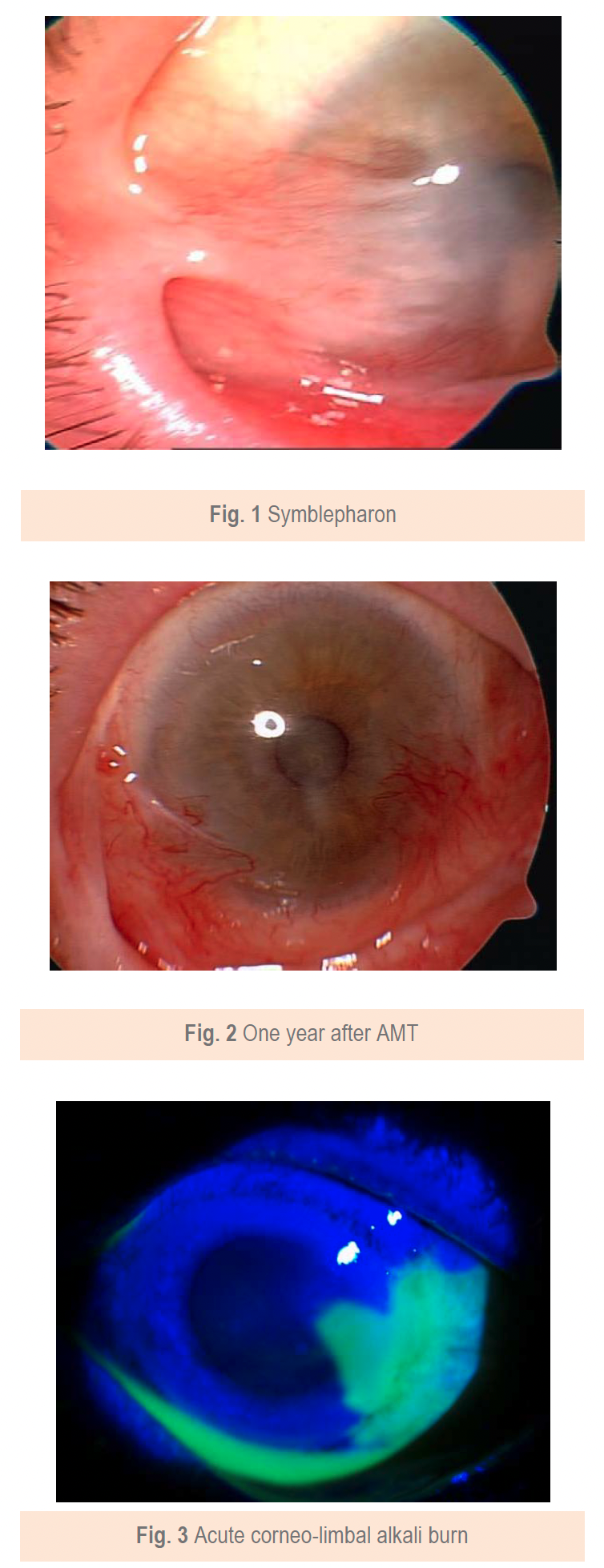
Good results were encountered in all 28 eyes. The anatomy of the cornea and conjunctiva was improved, with limited benefits only in old ocular burns, symblepharon (Fig. 1,2) and in one case of extended tumor of the cornea and conjunctiva. From 28 eyes, 23 (82%) also had a visual acuity improvement. The improvement was important in patients with a persistent epithelial defect and a recent/ acute alkali burn (Fig. 3,4), but the patients with old alkali burns and ocular tumors also had a benefit of 1 or 2 lines. The AMT BCVA ranged from LogMAR 0 to LogMAR 0.7. In our opinion, all the 28 patients had a good or improved cosmetic result, but only 26 were satisfied. Regarding the questionnaire, general discomfort symptoms improved in 25 patients, only one patient with symblepharon and 2 patients with tumors did not report an improvement. Photophobia was still present after AMT in 2 patients with old alkali burns (Fig. 5,6), 2 with symblepharon and 1 with ocular surface tumor, but the rest of 22 patients (78%) reported an improvement.
Conclusions
The amniotic membrane transplantation is a good and viable option in the ocular surface diseases and reconstruction. Its properties and its function as a substrate for cultivating limbal epithelial corneal cells, opens a new era of regenerative medicine, giving hope to patients with poor prognosis.
References
1. Holland EJ, Schwartz GS. Changing Concepts in the Management of Severe Ocular Surface Disease over Twenty-five Years. Corneea. September 2000; 19(5):688-698.
2. Gipson IK. The Ocular surface: The Challenge to Enable and Protect Vision. Invest Ophthalmol Vis Sci. 2007 October; 48(10): 4390–4398.
3. Meller D, Pauklin M, Thomasen H, Westekemper H, Steuhl KP. Amniotic Membrane Transplantation in the Human Eye. Dtsch Arztebl Int. 2011; 108(14): 243–8.
4. Shimazaki J, Yang HY, Tsubota K. Amniotic membrane transplantation of
ocular surface reconstruction in patients with chemical and thermal burns. Ophthalmology. 1997; 104:2068–2076.
5. Seitz B. Amniotic membrane transplantation. An indispensable therapy option for persistent corneal epithelial defects. Ophthalmology. 2007; 104: 1075–9.
6. Lee SB, Li DQ, Tan DT, Meller DC, Tseng SC. Suppression of TGF beta signaling in both normal conjunctival fibroblasts and pterygial body fibroblasts by amniotic membrane. Curr Eye Res. 2000; 20:325–34.
7. Tseng SC, Espana EM, Kawakita T et al. How does amniotic membrane work?. Ocul Surf. 2004; 2:177–87.
8. Shortt AJ, Secker GA, Notara MD et al. Transplantation of ex vivo cultured limbal epithelial stem cells: a review of techniques and clinical results. Surv Ophthalmol. 2007; 52:483–502.
9. Ganger A, Vanathi M, Mohanty S, Tandon R. Long-Term Outcomes of Cultivated Limbal Epithelial Transplantation: evaluation and Comparison of Results in Children and Adults. Biomed Res Int. 2015; 2015:480983.
Fig. 4 Four months after AMT
Fig. 5 Old alkali burn with corneal neovascularization
Fig. 6 Two months after AMT